
Perspective of tumor heterogeneity for treatments of intrahepatic cholangiocarcinoma with intrahepatic lithiasis
 0
0
Abstract
The heterogeneity of tumors results in significantly distinct biological characteristics of intrahepatic cholangiocarcinoma (ICC) caused by different etiologies. Among them, ICC caused by intrahepatic lithiasis (IHL-ICC) presents challenges in early detection, tumor staging, and surgical treatment, and has the poorest prognosis among all etiologies of ICC patients. Thus, it is essential to focus on early assessment of the possibility of developing ICC, prompt intervention of intrahepatic lithiasis, anatomical resection of hepatic parenchyma corresponding to the branch of the intrahepatic bile duct undergoing cancerous transformation, and enhanced postoperative follow-up of hepatolithiasis and ICC for IHL-ICC patients. These interventions are crucial to improve the clinical outcomes and overall survival of IHL-ICC patients.
Keywords
INTRODUCTION
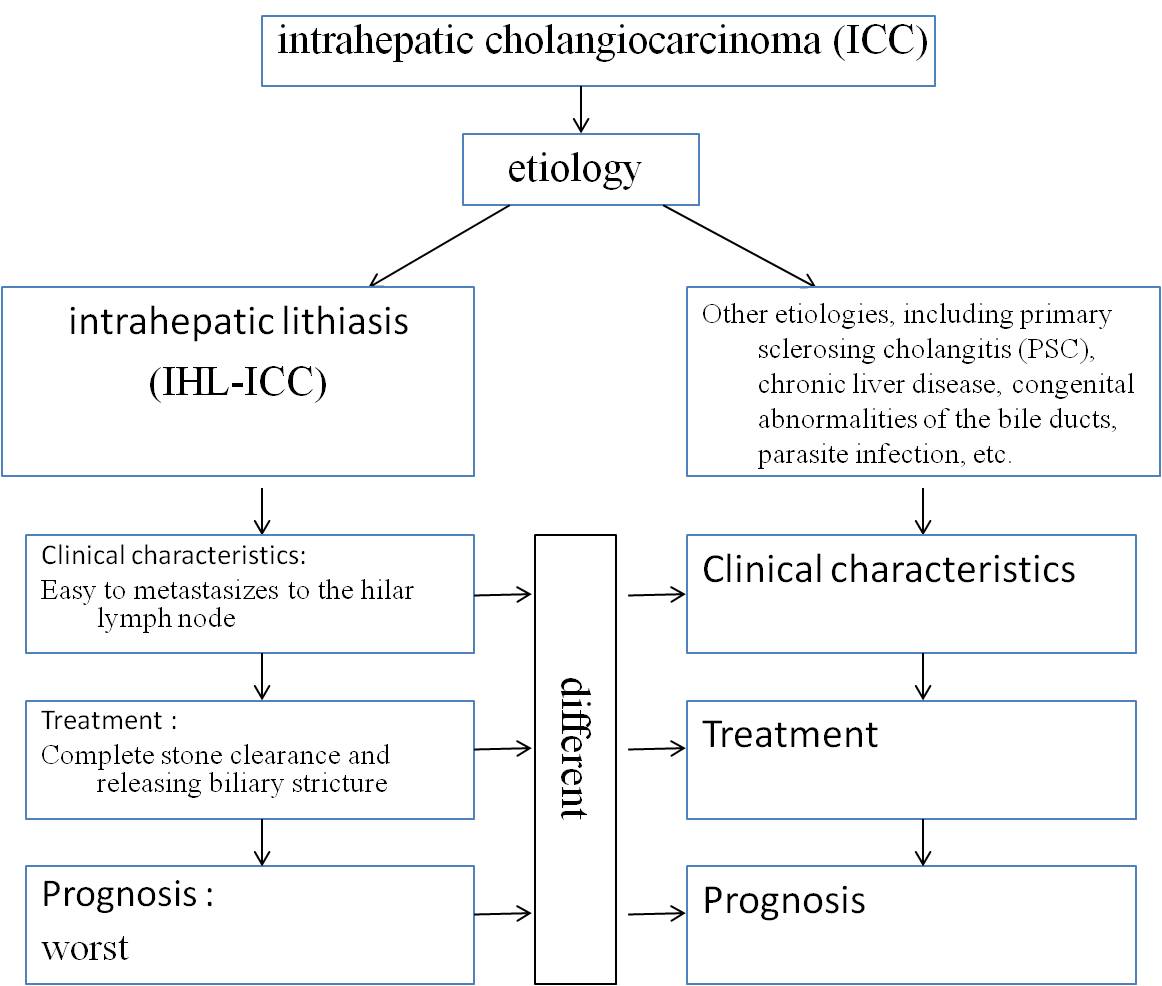
Intrahepatic cholangiocarcinoma (ICC) has emerged as a growing concern worldwide due to its increasing incidence and high mortality rates over the past few decades. Intrahepatic lithiasis, primary sclerosing cholangitis (PSC), chronic liver disease, congenital abnormalities of the bile ducts, parasite infection, and toxic exposures have all been associated with an increased risk of ICC[1]. However, the pathogenic factors contributing to ICC differ significantly by region. PSC is prevalent in the West, while hepatitis B and intrahepatic lithiasis (IHL) are more commonly implicated in the Asia Pacific region. It is important to note that the clinical manifestations and prognosis of ICC can vary greatly depending on the underlying cause. Recent evidence[2-4], coupled with our clinical experience, suggests that ICC caused by IHL (IHL-ICC) has the worst prognosis due to the heterogeneity of tumors. Therefore, I would like to explore how to improve the treatment of IHL-ICC here.
Pathogenic factors should be one of the important approaches in the classification of ICC
In all clinical practice guidelines for ICC[5-7], etiology is considered solely as a risk factor of ICC, rather than a basis for classification. However, there are significant differences in clinical characteristics and prognosis among ICC of various causes. For example, ICC caused by hepatitis B is predominantly of mass-forming type, and its clinical manifestations are similar to hepatocellular carcinoma (HCC)[8], which rarely metastasizes to the hilar lymph node. However, distinguished from HCC and ICC caused by hepatitis B, the majority of ICC are prone to lymph node metastasis. Furthermore, the prognosis of IHL-ICC patients was significantly worse than those of conventional ICC and HBV-ICC in many recent studies[2-4], including a Chinese study of 448 ICC patients[2] and a multi-institutional study[3]. However, these are all retrospective studies, and we need large-scale prospective cohort studies to further confirm the worse prognosis of IHL-ICC and the possible causes.
Previous studies have shown that cholangiocytic differentiation can divide ICC into two types with different etiologies, clinical manifestations, and molecular pathogeneses[9]. Moreover, integrated systems biology, which includes combinations of genomic, transcriptome, metabolome, protein, epigenetic, and chromosomal analyses, has been recommended for classifying heterogenous ICC subtypes[10].
These pieces of evidence all show that the heterogeneity of ICC is highly significant. Therefore, I suggest incorporating the factor of etiology into the classification of ICC.
To explore every possible avenue to improve the early diagnosis of IHL-ICC
As we all know, early diagnosis of tumors is crucial for improving their prognosis, especially for fatal tumors such as ICC. Previous studies have reported that about 2.3% to 13.0% of hepatolithiasis patients eventually developed cholangiocarcinoma[11]. The progression of cholangitis to ICC is a long process, and detecting IHL-ICC in its early stages is challenging. Liver enhancement imaging, serum carcinoembryonic antigen (CEA), and cancer antigen 19-9 (CA 19-9) are commonly used to detect the cholangiocarcinoma in hepatolithiasis patients. However, despite the use of Positron Emission Tomography (PET) imaging, the preoperative diagnostic accuracy of IHL-ICC is still low, ranging from 30% to 65%, due to concomitant chronic inflammation and necrosis caused by the presence of calculi. In my latest research[11], several commonly used clinical indicators were screened by using machine learning algorithms. Clinical physicians can conveniently use the tool to predict early IHL-ICC via a web page at http://www.bioinformatics.com.cn/calculate_7_factor_nomogram_total_points_for_zeng. The accuracy of the tool in predicting ICC is more than 82%. More research methodologies and specimens are being explored to uncover diagnostic indicators for ICC, such as oncogenes, tumor-suppressor genes, microRNAs, DNA methylation, protein and metabolic chemicals in bile, bile extracellular vesicles, and volatile organic compounds[12,13]. These new detection methods are expected to further the early identification of ICC.
ICC clinical staging system is not suitable for most cases of IHL-ICC. IHL-ICC is often mixed with intrahepatic cholangitis, even liver abscesses, and inflammatory enlargement of lymph nodes. As a result, it is difficult for clinical physicians to determine the actual size of the tumor and lymph node metastasis. Strengthening follow-up procedures for all patients with IHL and ensuring early detection of intrahepatic bile duct cancer are, therefore, of utmost importance.
Treatment of IHL-ICC
Surgical treatment
Radical resection surgery remains the primary treatment for IHL-ICC without distant metastasis. Complete stone clearance and releasing biliary stricture can prevent the development of ICC. In cases where intrahepatic lithiasis is concentrated in a specific liver lobe, such as frequently accumulating in the left lateral lobe or right posterior lobe of the liver, local atrophy of the affected lobe may occur, necessitating the resection of the entire lobe where the stones are located. Regional lymphadenectomy should be considered a standard part of surgical therapy for patients undergoing radical resection surgery. Liver transplantation is considered an optional treatment modality for early IHL-ICC without lymph node metastasis. However, due to the scarcity of suitable liver donors and the frequent occurrence of peritoneal adhesions in patients with IHL-ICC, liver transplantation surgery becomes challenging.
Adjuvant therapy after surgery
The recurrence rate of IHL-ICC following curative-intent surgery remains very high, which prompts a much greater need to develop and support novel strategies for adjuvant chemo- and targeted agent therapeutic trials. Like other types of ICC, adjuvant capecitabine, gemcitabine and oxaliplatin might be beneficial for resected ICC patients, but this has not yet been confirmed by recent research[14].
After IHL-ICC surgery, preservation of liver function is also crucial. Administering drugs that protect hepatocytes and promote bile secretion effectively improves liver function. In cases of biliary obstruction caused by stone blockage or bile duct stenosis, choledochoscopy or percutaneous transhepatic biliary drainage (PTCD) can be employed to relieve the obstruction and protect liver function. For patients with biliary tract infections, in addition to successful bile drainage after obstruction removed, the administration of antibiotics may be necessary for treatment.
Medical treatment for inoperable IHL-ICC patients
For unresectable IHL-ICC, besides the routine preservation of liver function, bile drainage, antibiotic therapy, and traditional chemotherapy, molecular targeted therapy and immunotherapy guided by Next-Generation Sequencing Solid Tumor are of paramount importance. IDH, FGFR, Immune Checkpoint Inhibitors, and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) are the possible useful medicines for the treatment of inoperable IHL-ICC[14].
CONCLUSION
Due to the heterogeneity of tumors, the clinical characteristics of IHL-ICC are different from those caused by other etiologies. It is recommended to use artificial intelligence methods to early predict ICC for patients with IHL. During the radical resection surgery, it is also necessary to remove intrahepatic stones as much as possible to relieve bile duct stenosis. If the accumulation of stones leads to atrophy of the liver segment, the liver segment should be removed. If possible, liver transplantation may be a more effective method for treating early IHL-ICC without lymph node metastasis.
DECLARATIONS
Authors’ contributionsMade substantial contributions to the conception and design of the study and performed data analysis and interpretation: Hou W, Zeng Q
Conception, design, and administrative support: Zheng M
Made substantial contributions to data collection, analysis and interpretation: Tu Y
Availability of data and materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestAll authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2023.
REFERENCES
1. Zhang H, Yang T, Wu M, Shen F. Intrahepatic cholangiocarcinoma: epidemiology, risk factors, diagnosis and surgical management. Cancer Lett 2016;379:198-205.
2. Li Q, Chen C, Su J, et al. Recurrence and prognosis in intrahepatic cholangiocarcinoma patients with different etiology after radical resection: a multi-institutional study. BMC Cancer 2022;22:329.
3. Zhang XF, Chakedis J, Bagante F, et al. Implications of intrahepatic cholangiocarcinoma etiology on recurrence and prognosis after curative-intent resection: a multi-institutional study. World J Surg 2018;42:849-57.
4. Wang Q, Li J, Lei Z, et al. Prognosis of intrahepatic cholangiocarcinomas with hbv infection is better than those with hepatolithiasis after R0 liver resection: a propensity score matching analysis. Ann Surg Oncol 2017;24:1579-87.
5. Amin MB. American Joint Committee on Cancer, American Cancer Society. AJCC cancer staging manual. Eight edition. Chicago, IL: American Joint Committee on Cancer, Springer; 2017. xvii 1024.
6. Weber SM, Ribero D, O'Reilly EM, Kokudo N, Miyazaki M, Pawlik TM. Intrahepatic cholangiocarcinoma: expert consensus statement. HPB 2015;17:669-80.
7. Kubo S, Shinkawa H, Asaoka Y, et al. Liver cancer study group of Japan clinical practice guidelines for intrahepatic cholangiocarcinoma. Liver Cancer 2022;11:290-314.
8. Zhou H, Wang H, Zhou D, et al. Hepatitis B virus-associated intrahepatic cholangiocarcinoma and hepatocellular carcinoma may hold common disease process for carcinogenesis. Eur J Cancer 2010;46:1056-61.
9. Liau JY, Tsai JH, Yuan RH, Chang CN, Lee HJ, Jeng YM. Morphological subclassification of intrahepatic cholangiocarcinoma: etiological, clinicopathological, and molecular features. Mod Pathol 2014;27:1163-73.
10. Wang XW, Thorgeirsson SS. The biological and clinical challenge of liver cancer heterogeneity. Hepat Oncol 2014;1:349-53.
11. Shen X, Zhao H, Jin X, et al. Development and validation of a machine learning-based nomogram for prediction of intrahepatic cholangiocarcinoma in patients with intrahepatic lithiasis. Hepatobiliary Surg Nutr 2021;10:749-65.
12. Bao F, Liu J, Chen H, Miao L, Xu Z, Zhang G. Diagnosis biomarkers of cholangiocarcinoma in human bile: an evidence-based study. Cancers 2022;14:3921.
13. Liu XF, Tang K, Sui LL, Xu G. Cholangiocarcinoma: present status and molecular aspects of diagnosis. Oncol Res 2014;22:177-83.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Hou W, Tu Y, Zheng M, Zeng Q. Perspective of tumor heterogeneity for treatments of intrahepatic cholangiocarcinoma with intrahepatic lithiasis. Hepatoma Res 2023;9:35. http://dx.doi.org/10.20517/2394-5079.2023.40
AMA Style
Hou W, Tu Y, Zheng M, Zeng Q. Perspective of tumor heterogeneity for treatments of intrahepatic cholangiocarcinoma with intrahepatic lithiasis. Hepatoma Research. 2023; 9: 35. http://dx.doi.org/10.20517/2394-5079.2023.40
Chicago/Turabian Style
Hou, Wenjie, Yifan Tu, Minghua Zheng, Qiqiang Zeng. 2023. "Perspective of tumor heterogeneity for treatments of intrahepatic cholangiocarcinoma with intrahepatic lithiasis" Hepatoma Research. 9: 35. http://dx.doi.org/10.20517/2394-5079.2023.40
ACS Style
Hou, W.; Tu Y.; Zheng M.; Zeng Q. Perspective of tumor heterogeneity for treatments of intrahepatic cholangiocarcinoma with intrahepatic lithiasis. Hepatoma. Res. 2023, 9, 35. http://dx.doi.org/10.20517/2394-5079.2023.40
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 4 clicks
Cite This Article 4 clicks

 Like This Article 4
likes
Like This Article 4
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.