
Repeat laparoscopic anatomical liver resection in a hepatocellular carcinoma patient: a case report
 0
0Abstract
Anatomical resection (AR) has been reported to achieve better long-term outcomes than non-anatomical resection for the treatment of hepatocellular carcinoma (HCC). The surgical feasibility and oncological significance of laparoscopic AR (LAR), especially “subsegment resection”, “cone unit resection”, and repeat LAR for HCC, remain unproven. We present a 67-year-old patient with alcoholic liver cirrhosis and HCC who underwent full LAR three times, focusing on the technical aspects of the Glissonean approach. Repeating LAR for recurrent HCC could be a safe and feasible procedure. However, HCC recurred in the neighboring segment twice, even though pathological vascular invasion and marginal remnants were not confirmed. We should investigate the oncological significance and advancements in subsegmentectomy and cone unit resection, in the future.
Keywords
INTRODUCTION
Anatomical resection (AR) has been reported to achieve better long-term outcomes than non-anatomical resection for the treatment of hepatocellular carcinoma (HCC)[1,2]. Laparoscopic liver resection (LLR) has recently gained popularity because of its short-term advantages compared with open liver resection[3-7]. However, the surgical feasibility and oncological significance of laparoscopic AR (LAR), especially “subsegment resection,” “cone unit resection”, and repeat LAR for HCC, remain unproven[8].
We report the case of a patient with HCC who received full LAR three times, focusing on the technical aspects of the Glissonean approach. We all discuss the limitations of AR for HCC.
CASE PRESENTATION
Preoperative information
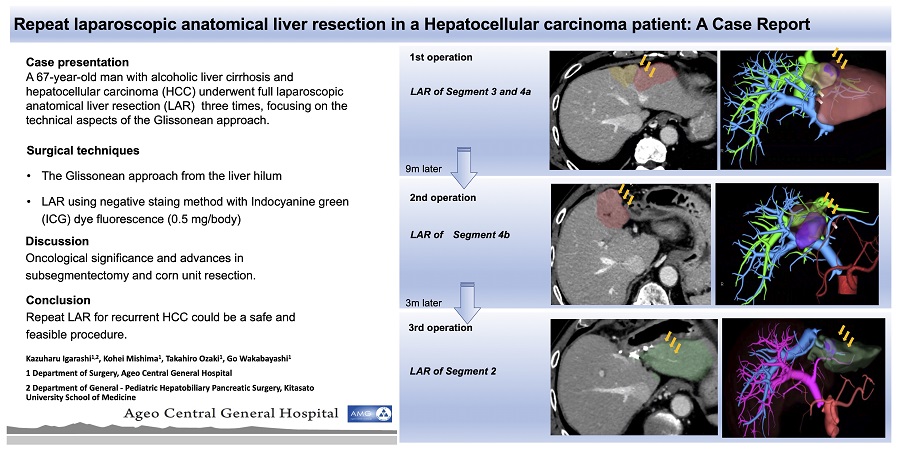
A 67-year-old man with alcoholic liver cirrhosis and no hepatitis B or C virus infection was referred to our hospital. Abdominal computed tomography (CT) showed a 3 cm liver mass in Segments 3 and 4a with the typical features of HCC with early arterial enhancement and portal vein washout, which was classified as LR-5 of the Liver Imaging Reporting and Data System (LI-RADS). Preoperative evaluation of the liver function revealed Child-Pugh class A and the 15 min retention rate of Indocyanine green (ICG15) was 11%. The serum levels of tumor markers for alpha-fetoprotein (AFP) and protein induced by vitamin K absence or antagonist-II (PIVKAII) were 67.7 ng/mL and 74 mAU/mL, respectively. Preoperative surgical simulation using three-dimensional (3D) CT rendered on a specific workstation (ZIOSTATION 2, Ziosoft Inc., Tokyo, Japan) suggested the feasibility of limited anatomical subsegmentectomy instead of left hepatectomy (resection volume was 115 mL, which was 9.7% of the total liver volume) on Makuuchi’s criteria.
Surgical techniques
The Glissonean approach from the liver hilum was applied to selectively isolate and finally close these pedicles for the segment or subsegment involved by the tumor. ICG dye fluorescence (0.5 mg/body) was used to obtain demarcation lines both superficially and in the deep parenchyma, achieving a true anatomical resection.
Course of treatment
We performed pure LAR of Segments 3 and 4a. The operative time was 264 min, the estimated blood loss was 5 mL, and there was no need for blood transfusion. The patient was discharged on Postoperative Day 6 without any postoperative complications. Pathological findings of the tumor proved stage II moderately differentiated HCC with negative resection margins and no vascular invasion [Figure 1].
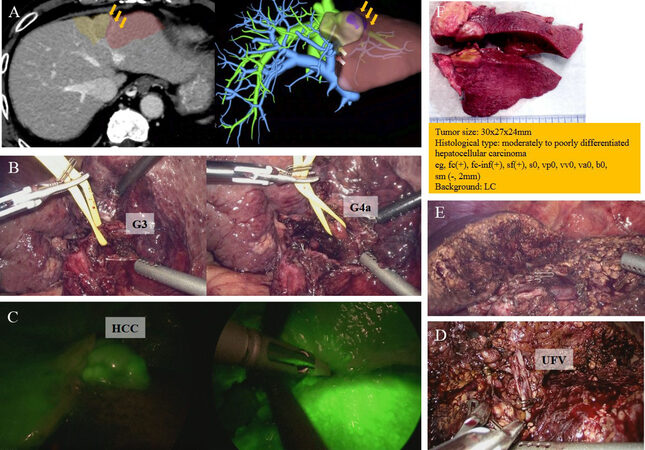
Figure 1. First operation: (A) preoperative 3D CT reconstruction; (B) Glissonean approach respecting Laennec’s capsule with isolation of Glissonean branches of Segments 3 (G3) (left) and 4a (G4a) (right); (C) HCC staining by ICG and superficial parenchymal resection along the demarcation line; (D) isolation of umbilical fissure vein (UFV) as drainage vein of Segments 3 and 4a; (E) surgical field after LAR of Segments 3 and 4a; and (F) macroscopic findings and pathological results. 3D CT, three-dimensional computed tomography; HCC, hepatocellular carcinoma; ICG, Indocyanine green; LAR, laparoscopic anatomical liver resection.
Nine months after the previous surgery, abdominal CT revealed recurrence, with two liver masses (1.5 and 1 cm), which were classified as LR-5 of LI-RADS located in Segment 4b. Liver function was Child-Pugh A and ICG15 was slightly elevated (23%). Serum levels of AFP and PIVKA-II were 67.8 ng/mL and 17 mAU/mL, respectively. We performed a second LAR of Segment 4b. The operative time was 195 min and the estimated blood loss was 28 mL. The patient was discharged on Postoperative Day 8 with no postoperative complications. Pathological findings showed stage II moderately differentiated HCC with negative resection margins and no vascular invasion [Figure 2].
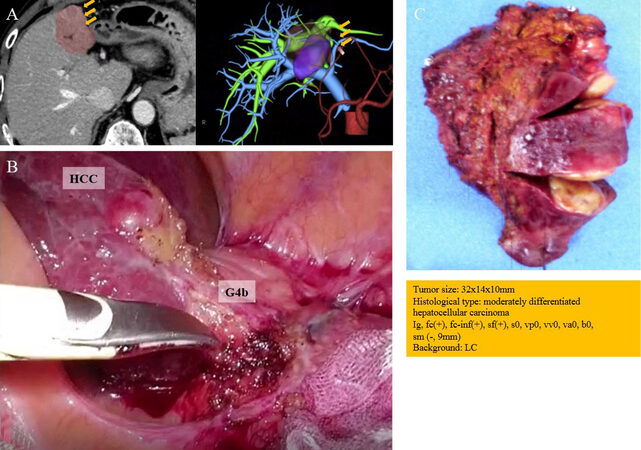
Figure 2. Second operation: (A) preoperative 3D CT reconstruction; (B) isolation of Glissonean branches of Segment 4b (G4b); and (C) macroscopic findings and pathological results. 3D CT, three-dimensional computed tomography.
Three months later, abdominal CT revealed recurrence, which was a 1.3 cm liver mass classified as LR-5 of LI-RADS located in Segment 2. ICG15 was not elevated (16%). Serum levels of AFP and PIVKA-II were 58.9 ng/mL and 20 mAU/mL, respectively. We performed a third LAR of Segment 2. The operative time and the estimated blood loss were 183 min and 60 mL, respectively. The patient discharged on Postoperative Day 7 with no postoperative complications. Pathological examination of the resection specimen proved stage II moderately differentiated HCC with negative resection margins and no vascular invasion [Figure 3]. The patient showed no recurrence during the follow-up, nine months after the third surgery.
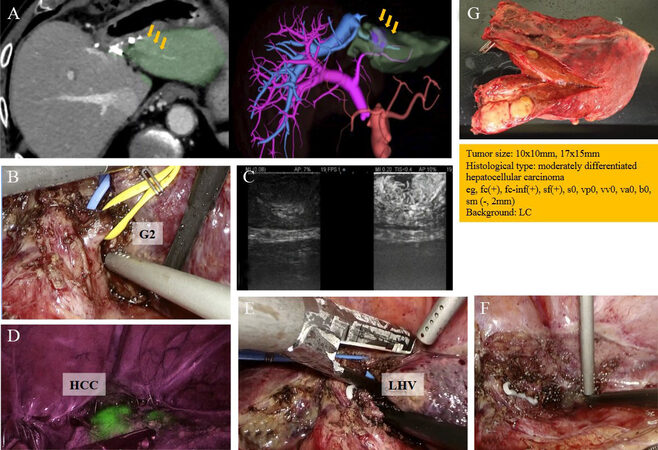
Figure 3. Third operation: (A) preoperative 3D CT reconstruction; (B) Glissonean approach respecting Laennec’s capsule with isolation of Glissonean branches of Segment 2 (G2); (C) intraoperative ultrasonography (IOUS); (D) HCC staining by ICG; (E) isolation of left hepatic vein (LHV) as drainage vein of Segment 2; (F) surgical field after LAR of Segment 2; and (G) macroscopic findings and micropathological results. 3D CT, three-dimensional computed tomography; HCC, hepatocellular carcinoma; ICG, Indocyanine green; LAR, laparoscopic anatomical liver resection.
DISCUSSION
In the treatment of HCC, eradication of intrahepatic metastasis with vascular invasion is one of the most important considerations. AR, taking into consideration both the preservation, to the maximum extent possible, of liver functional parenchyma and eradication of intrahepatic metastasis, would be a theoretically reasonable procedure[1]. In the present case, in which we performed anatomical resection, HCC recurred in the neighboring segment twice, even though pathological vascular invasion and marginal remnants were not confirmed. As a result, we performed a left lobectomy. This may suggest a limitation of cone unit resection and subsegmentectomy. The anatomical boundary between Segments 4a and 4b is extremely difficult to identify in appearance because there is no clear hepatic vein that serves as a landmark on the border, and the Glissonean branches from the umbilical portion of portal vein to Segment 4 show diversity and are often radial. Conversely, ICG visualizes difficult transection boundaries and ultimately allows for liver parenchyma-sparing anatomic resection of the exact cancer-bearing region[9]. In fact, ICG often revealed that the transection borders in the deep layer as intersegmental planes were not flat but uneven. Although the liver parenchyma-sparing anatomic resection was performed accurately with adequate margins for the present case, oncologic radicality may have been inadequate. We should study further the anatomy of Segment 4.
Despite no vascular invasion, detailed histopathological examination in our institution suggested that the recurrence patterns in this case were not multicentric occurrences based on liver cirrhosis but intrahepatic metastasis because the pathological structures of the specimen following three repeat resections were similar to each other in terms of differentiation. A genetic examination may be required to confirm the similarities for a definitive diagnosis. Many previous studies reported that, compared to major open liver resection, laparoscopic liver resection has short-term clinical advantages, including reduced blood loss, lower postsurgical morbidity, and shorter hospital stay for HCC, and the long-term oncological outcomes were comparable in both groups[10-12]. The oncological significance and advances in subsegmentectomy and cone unit resection should be investigated in the future.
Laparoscopic repeat LAR for recurrent HCC could be a safe and feasible procedure, as suggested by previous systematic reviews and meta-analysis[13-15]. We believe that the important points for making the next operation easier with a few adhesions of the abdominal wall and hilum of the liver include no extra mobilization, no ischemic area should be left by performing anatomical resection, to spray a spray-type anti-adhesion barrier (Ad Spray type L®, TERUMO Corp, Tokyo, Japan) on the remaining liver and hilum of the liver, and low intraoperative bleeding. In addition, the laparoscopic procedure might be good for the dissection of adhesion due to its magnification.
In conclusion, we report the case of a patient with HCC who received full LAR three times. Laparoscopic repeat LAR for recurrent HCC could be a safe and feasible procedure. We should investigate the oncological significance and advancements in subsegmentectomy and cone unit resection, in the future.
DECLARATIONS
Authors’ contributionsConceived and designed the manuscript: Go Wakabayashi
Wrote the manuscript: Kazuharu Igarashi
Critically revised the manuscript: Go Wakabayashi, Kohei Mishima, Takahiro Ozaki
Availability of data and materialsData supporting our Report are deposited in our database and are available at request via contat with our corresponding author.
Financial support and sponsorshipNone.
Conflict of interestAll authors declared that there no conflicts of interest.
Ethical approval and consent to participateAt our Institution, the day before surgery all patients sign an informed consent which comprehends data collection in anonymized form (video recording included), so no external ethical approval was necessary in this case.
Consent for publicationWritten informed consent was obtained from the patient before the surgery.
Copyright© The Author(s) 2022.
REFERENCES
1. Hasegawa K, Kokudo N, Imamura H, et al. Prognostic impact of anatomic resection for hepatocellular carcinoma. Ann Surg 2005;242:252-9.
2. Haruki K, Furukawa K, Fujiwara Y, et al. Effectiveness of anatomical resection for small hepatocellular carcinoma: a propensity score-matched analysis of a multi-institutional database. J Gastrointest Surg 2021;25:2835-41.
3. Wakabayashi G. What has changed after the Morioka consensus conference 2014 on laparoscopic liver resection? Hepatobiliary Surg Nutr 2016;5:281-9.
4. Kaneko H, Otsuka Y, Kubota Y, Wakabayashi G. Evolution and revolution of laparoscopic liver resection in Japan. Ann Gastroenterol Surg 2017;1:33-43.
5. Takahara T, Wakabayashi G, Konno H, et al. Comparison of laparoscopic major hepatectomy with propensity score matched open cases from the National Clinical Database in Japan. J Hepatobiliary Pancreat Sci 2016;23:721-34.
6. Twaij A, Pucher PH, Sodergren MH, Gall T, Darzi A, Jiao LR. Laparoscopic vs open approach to resection of hepatocellular carcinoma in patients with known cirrhosis: systematic review and meta-analysis. World J Gastroenterol 2014;20:8274-81.
7. Cherqui D, Laurent A, Tayar C, et al. Laparoscopic liver resection for peripheral hepatocellular carcinoma in patients with chronic liver disease: midterm results and perspectives. Ann Surg 2006;243:499-506.
8. Imura S, Yamada S, Saito Y, Ikemoto T, Morine Y, Shimada M. Utility of cone unit liver resection for small hepatocellular carcinoma: a propensity score matched analysis. HPB (Oxford) 2021;23:739-45.
9. Berardi G, Igarashi K, Li CJ, et al. Parenchymal sparing anatomical liver resections with full laparoscopic approach: description of technique and short-term results. Ann Surg 2021;273:785-91.
10. Takahara T, Wakabayashi G, Beppu T, et al. Long-term and perioperative outcomes of laparoscopic versus open liver resection for hepatocellular carcinoma with propensity score matching: a multi-institutional Japanese study. J Hepatobiliary Pancreat Sci 2015;22:721-7.
11. Wakabayashi G. Systematic reviews from the 2nd international consensus conference on laparoscopic liver resection. J Hepatobiliary Pancreat Sci 2015;22:325-6.
12. Wang ZY, Chen QL, Sun LL, et al. Laparoscopic versus open major liver resection for hepatocellular carcinoma: systematic review and meta-analysis of comparative cohort studies. BMC Cancer 2019;19:1047.
13. Morise Z. Status and perspective of laparoscopic repeat liver resection. World J Hepatol 2018;10:479-84.
14. Onoe T, Yamaguchi M, Irei T, et al. Feasibility and efficacy of repeat laparoscopic liver resection for recurrent hepatocellular carcinoma. Surg Endosc 2020;34:4574-81.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Igarashi K, Mishima K, Ozaki T, Wakabayashi G. Repeat laparoscopic anatomical liver resection in a hepatocellular carcinoma patient: a case report. Hepatoma Res 2022;8:21. http://dx.doi.org/10.20517/2394-5079.2022.02
AMA Style
Igarashi K, Mishima K, Ozaki T, Wakabayashi G. Repeat laparoscopic anatomical liver resection in a hepatocellular carcinoma patient: a case report. Hepatoma Research. 2022; 8: 21. http://dx.doi.org/10.20517/2394-5079.2022.02
Chicago/Turabian Style
Igarashi, Kazuharu, Kohei Mishima, Takahiro Ozaki, Go Wakabayashi. 2022. "Repeat laparoscopic anatomical liver resection in a hepatocellular carcinoma patient: a case report" Hepatoma Research. 8: 21. http://dx.doi.org/10.20517/2394-5079.2022.02
ACS Style
Igarashi, K.; Mishima K.; Ozaki T.; Wakabayashi G. Repeat laparoscopic anatomical liver resection in a hepatocellular carcinoma patient: a case report. Hepatoma. Res. 2022, 8, 21. http://dx.doi.org/10.20517/2394-5079.2022.02
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 5 clicks
Cite This Article 5 clicks

 Like This Article 33
likes
Like This Article 33
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.